

Definition Sleeve Gastrectomy
It is about a technique of Surgery of obesity known as “bariatric.
It aims at the obese weight loss of the patients.
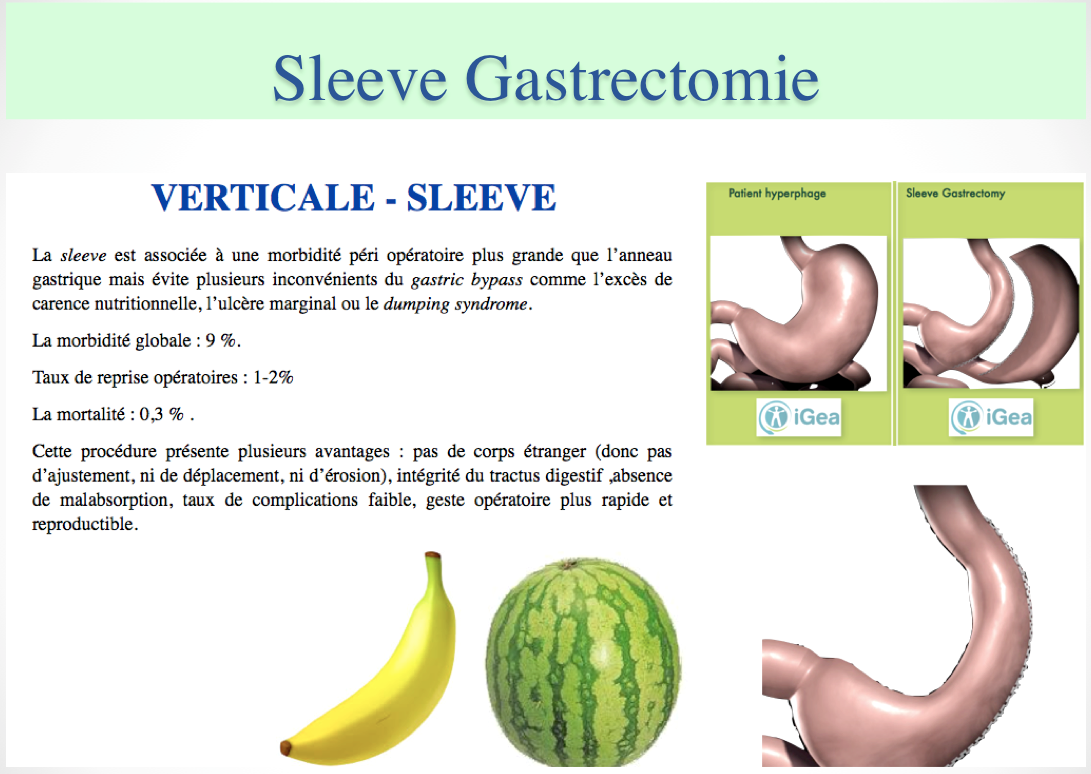
Sleeve Gastrectomy is a restrictive surgical procedure suggested to the patients hyperphages (who eat much at the time of the meals).
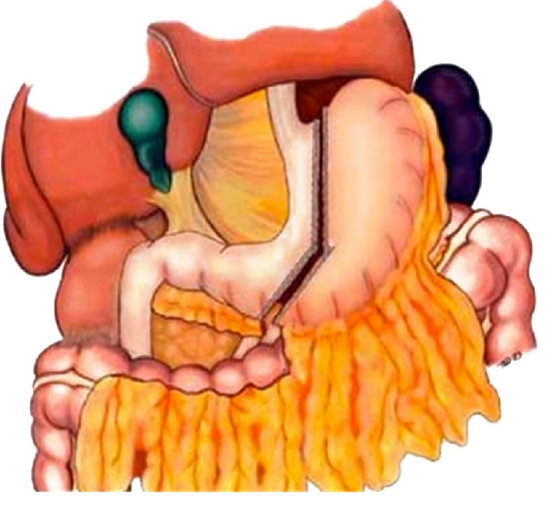
Sleeve gastrectomy consists in reducing the gastric capacity
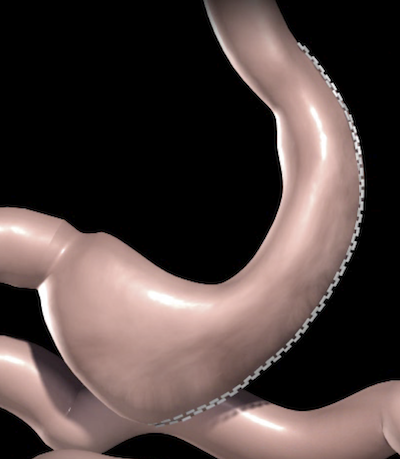
One removes the 2/3 of gastric volume definitively and one leaves a stomach in the shape of tube thanks to a fastening (section) on all the height of the great gastric curve (approximately 25 to 30 cm).
The operational part is entrusted to the anatomopathologists for the analysis.
The size of the stomach which is left in place is variable according to the tube of calibration. This candle is introduced during the operation by the mouth into the oesophagus and the stomach by the anaesthetists. We used a candle of 34 Fr (gauges in the neighbourhoods 2 cm in diameter) which ensures a maximum of regularity in the clothes industry of the line of fastening.
- To Note
- The volume of the remaining stomach is about 100-150 ml after the operation (size of a banana)
- The procedure is carried out under coelioscopy-laparoscopy with 3 sometimes 4 incisions: 1-2 of 5 mm, two of 12 mm (of which one can be widened to allow the extraction of the stomach in a bag = endobag).
- Systematic Pas de external drainage
- A hormonal effect due to the complete resection of the fundus contributes to make effective Sleeve Gastrectomie: the cells which secrete the hormone stimulating the appetite (ghréline) are removed with the fundus
- bibliography ( link)
SLEEVE GASTRECTOMY IS A STOMACH – WATERMELON THAT BECOMES STOMACH – BANANA
dr SALSANO Vincenzo
- . .
| Definition Sleeve Gastrectomy Dr Vincenzo Salsano update Février 2020 |
|---|
Advantages of Sleeve Gastrectomy

Advantages of Sleeve Gastrectomy are the following:
1- Intervention generally made completely under laparoscopy (coelioscopy).
- Security level comparable with the ring with a low conversion rate (even at the super-obese patients, of male sex).
2 – It does not have there an installation of foreign body, contrary to the gastric ring.
- The staples used are generally well integrated at the end of a few months: they are identical to those used in any other abdominal surgery.
3- The sleeve gastrectomy does not cause any malabsorption.
- It is about a very physiological intervention.
- There is no modification moreover digestive tract, nor of digestion.
- Sleeve Gastrectomie does not generate a deficiency in vitamins.
- There is no impact on the effectiveness and the proportioning of your treatments (if you take medicines or the contraceptive pill).
- The digestive tract remains accessible to any endoscopic investigation.
- There is no dumping syndrome précoce* or tardif*.
4- Food comfort is better compared to the gastric ring (link), because there is not the feeling of blocking with frequent vomiting.
{kind=link}
- In the sleeve gastrectomy, the reduction of gauge (volume) of the stomach is regular along the tube: a food quasi-normal, although of reduced quantity, is possible. Bibliography
5- There are not the risks related to the seams (anastomoses) digestive: pas de anastomotic dents and of late strictures, unlike By-pass.
6- Il n’y a pas les risques de reprise opératoire pour hernie interne à long terme, à la différence du By-pass.
7- La sleeve gastrectomie permet de traiter les comorbidités liés à l’obésité avec une efficacité comparable au Gastric By-Pass
Disappearence and/or control of
- diabetes
- hypertension
- Ostructive sleep apnea syndrome,
- dyslipidemy .
8- The results in terms of weight loss appear higher than those which the installation of a gastric ring can ensure and are comparable with those of an operation more sophisticated like Gastric. bibliography
9- Sleeve Gastrectomie is an evolving operation, at least as much as the ring: in the event of resumption of weight or insufficient weight loss we can associate Gastric By-pass or a bilio-pancreatic derivation.

| Advantages of Sleeve gastrectomy Dr Vincenzo Salsano update Novembre 2016 |
|---|
Results of Sleeve Gastrectomy
The data published concerning Sleeve Gastrectomie show very interesting results in the medium term (3 years).
In the experiment montpelliéraine, the loss of excess of weight was higher than 65% with a three years passing and control, even disappearance, Co-morbidities was comparable with Gastric By-pass.
These figures are very encouraging but it should be specified that the true value on the weight loss of any intervention of bariatric surgery is generally appreciated five years after the operation.

We evaluate the weight loss with each consultation in term of
- % EWL (percentage of excess of lost weight).
- % EBL (percentage of lost excess of IMC).
The medium-term weight loss (3 years) is estimated at more than 60% of the excess of weight (% EWL) and at more than 75% of excess of IMC (%EBL).
- Here the example of a patient obese, diabetic, operated of Sleeve Gastrectomy it there 3 years.
- Currently it weighs 75 kg: it is not diabetic any more and is declared very satisfied with its result and its quality of life
- Here parameters before Sleeve Gastrectomie:
Size: 1.67 m; Weight: 120 kg; Ideal weight according to Lorentz: 60 kg.
Excess of weight (to be lost): 60 kg. ; IMC (in English BMI): 43 Kg/m ².
IMC ideal: 22.5 Kg/m ²; Excess of IMC: (43-22,5) = 20.5.
Standard diabetes II.
Results at 5 years of the intervention:
Weight: 75 kg; Size: 1.67 m; Lost weight: 45 kg.
IMC: 26,8 Kg / m ².
% EWL = (45 kg perdus / 60kg di essere persi) = 75%.
% EBL = (43 -26,8 / 20,5) = 79%.
Disappearance of the diabetes..
TESTIMONY EFFECTIVENESS SLEEVE GASTRECTOMIE A’ 18 MONTHS
%EWL = 100% = loss of 52 kg excess of weight 52 kg
Percentage of excess weight loss ( % EWL )
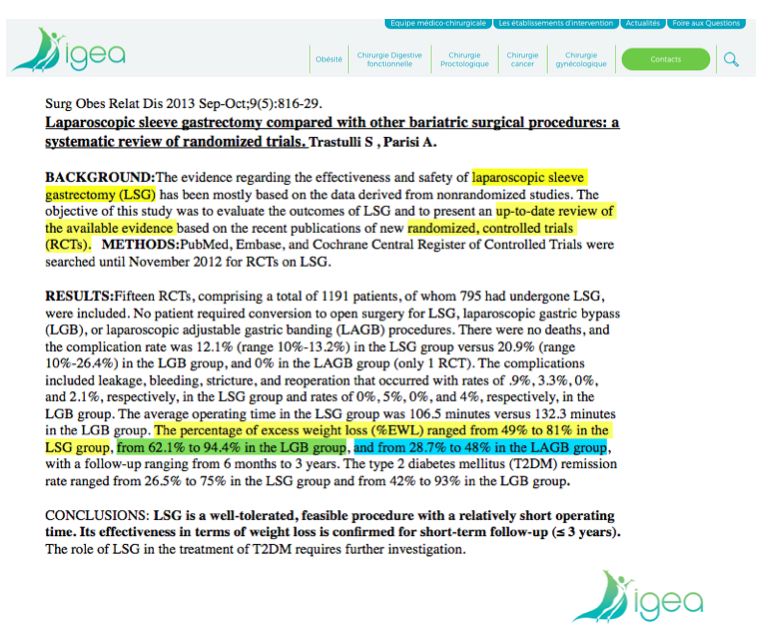
Comparison Laparoscopic Sleeve Gastrectomy – LSG- versus Laparoscopic Gastric By Pass en Y- LRYGB
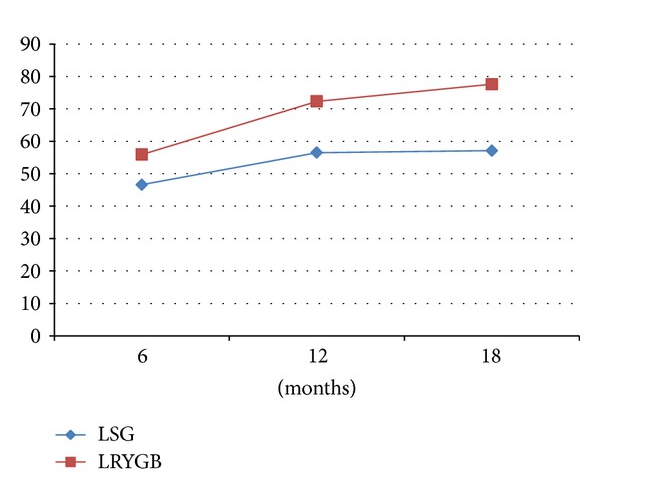
Percentage of the exces of weight ( % EWL ) LSG vs LRYGB vs LAGB
Comparison Laparoscopic Sleeve Gastrectomy – LSG- versus Laparoscopic Gastric By Pass en Y- LRYG B versus LABG
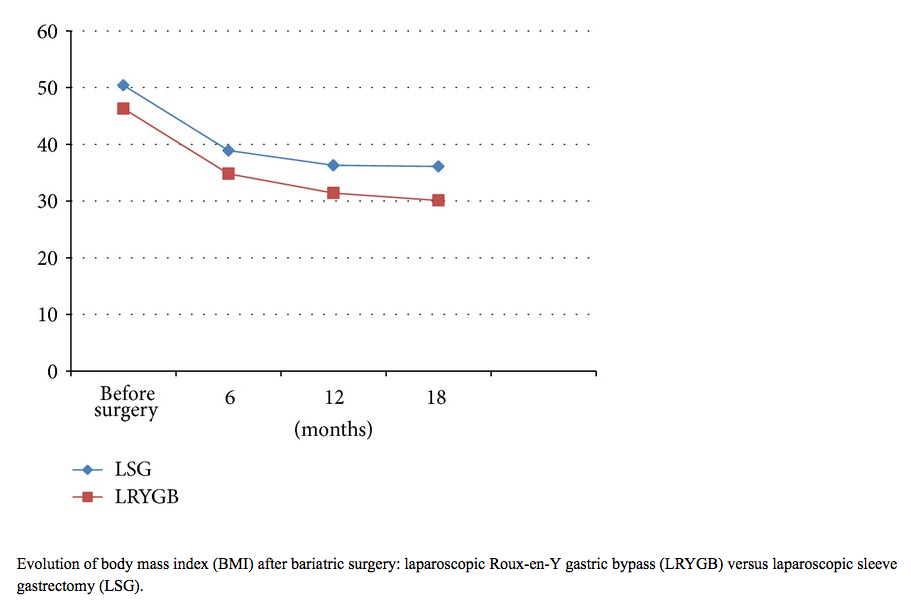
Percentage of body mass index ( BMI ) lost ( % PIP )
| Les Résultats de la Sleeve Gastrectomie dr Vincenzo Salsano mise à jours Novembre 2016 |
|---|
Complications of Sleeve Gastrectomy
The Fistula Is the more frightening postoperative complication
It is about an escape of digestive liquid on the level of the line of fastening (leaks products of contrast to the oral opacifying in TOGD/scanner). The formation of an abscess under diaphragmatic left, the clinical picture of peritonitis or the early haemorrhage generally require the surgical reintervention in the first 24-28 hours..
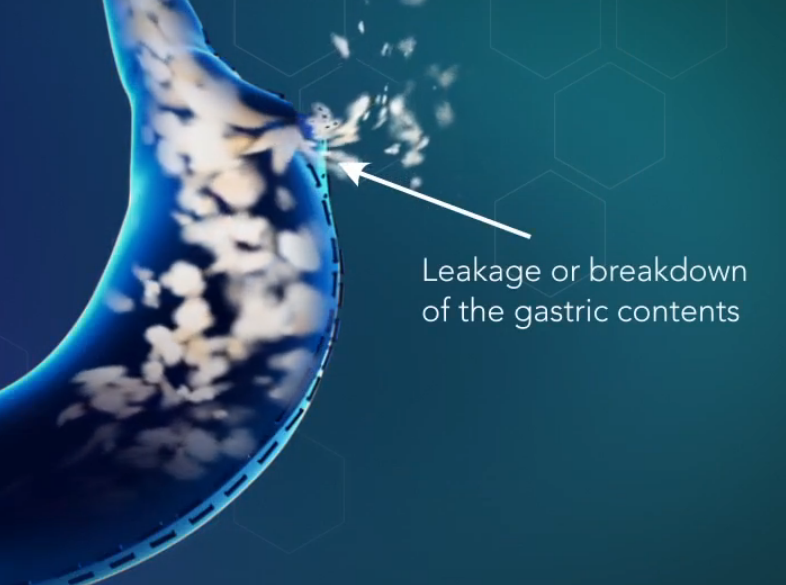
- Fistula ( link pubmed ) : the rate is an average of 3 %.
- The obese super patients (IMC >50 KG/m2) with antecedents of gastric ring are more at the risk of dent
- This rate is appreciably lower (1%) in the sub-group of the patients operated for the first time with a severe or morbid obesity (and not being super-obese: IMC < 50Kg/m ²).
- The fistula lengthens the time of hospitalization (one or more D operation can be made necessary!!! )
- The time of cicatrization is variable and very difficult to predict with certainty because it depends on many parameters.
- The obese super patients (IMC >50 KG/m2) with antecedents of gastric ring are more at the risk of dent
Early post-operative haemorrhage
- rate 2,5% ; bleeding : staple , orifices of trocar , spleen and gastro-splenic ligament
Stenosis
It is about contracting on the level of the remaining stomach: this risk is estimated at approximately 3%. It is cause of vomiting prolonged in time
Reflux gastro-œsophageal
- 20% of the patients can present a Backward flow gastro œsophagien in the immediate continuations of a sleeve.
- The symptoms are treated by IP (omeprazole, Pantoprazole) with a good answer
- This RGO tends to decrease, to even disappear with the weight loss from the patient
- In the event of severe RGO Gastric By-pass in Y can be carried out
- During the intervention, it is necessary to gauge well the longitudinal gastrectomy with a tube To mow
- In spite of the use of a candle of calibration, the line of staples can present irregularities (aspect bored with the gastroscopy), a rupture has minimum fastening can pass unperceived and support the appearance of a contracting.
- If the problems of daily vomiting are not regulated with an endoscopic dilation, a new remote surgical operation becomes necessary.
- RGO: The Symptoms of backward flow gastro-œsophagien are present at 1/3 of the patients but are well controlled with the medical care..
- The mortality of this intervention is quasi worthless (0,1%)
- We estimate at the present time that the operation of Sleeve Gastrectomie, if it is carried out by team expert, presented a very high security level with a low total morbidity ) ( bibliography )
TRAITMENT OF A FISTULA AFTER SLEEVE GASTRECTOMY
WHATCH THE VIDEO TESTIMONIAL
- Woman in morbid obesity: 112 kg for a size of 1m 65; IMC 41 Kg/m2 46 kg (ideal weight 65 kg) operated of a sleeve gastrectomy
- Appearance of a collection (infected bruise) with J5 without obviousness of FISTULA to the scanner
- Operational resumption with J7: evacuation bruise, washing, drainage (opening of the fistula not found) and installation of a PEAK line
- Control of the septic state with antibiotherapy, (left in home medical care; no oral food)
D hospitalization in J90: - A) description of a residual collection in communication with the sinus opening (to scan with oral opacifying in ventral position.
- B) Operational recovery by laparotomy: drainage in aspiration (standard VAC), installation of nutritional jejunostomy
- C) Cure of the fistula with J180 = the patient took again a food split, normal 9 months after the operation!!! !
- To NOTE
- LThe cure is defined like the closing of the dent in absence of symptoms .
Tardive complications of Sleeve Gastrectomy
- Dilatation of the gastric tube and probable weight regain
DILATION OF THE GASTRIC TUBE
- It is probably related on a defect or a too broad calibration to the beginning
If all the large tuberosity were removed by producing a narrow tube, dilation in time is not very probable since the muscle fibres of the small curve are not very extensible - On the other hand, a too broad gastric tube on the level proximal (by leaving an aspect diverticulaire dissolves) could theoretically predispose with this complication.
- This aspect is found sometimes in the reintervention of sleeve gastrectomy after failure of ring.
Weight regain
It is difficult to allot the recovery to a dilation of the gastroplastie which remains a rare event; in addition important slimmings were obtained with a relatively broad calibration (48 Fr in experiment BPD/SL)
The resumption of weight is rather put on a dietetic deviance with a food very heating with a pasty texture /lisse (milk shake), doubled of an absence of physical-activity.
| Complications de la Sleeve Gastrectomie Dr Vincenzo Salsano mise à jour Novembre 2016 |
|---|
Rational of the weight loss obtained with Sleeve Gastrectomy
How does one lose weight with Sleeve Gastrectomy?
- Reduction food supply
- You will eat less = small of the neo stomach = the gastric tube has the shape of a banana with a capacity reduced to 150 DC or ml (1 pot of Yoghourt)
- You will be less hungry = hormonal effect = reduction of the plasmatic rate of the ghréline which is at the present time the only hormone known orexigene. The ghréline is a peptide of 28 amino-acids secreted mainly by the stomach at the peripheral level, but also by the pituitary gland and the hypothalamus in the brain.
SLEEVE GASTRECTOMY IS A STOMACH – WATERMELON THAT BECOMES STOMACH – BANANA
dr SALSANO Vincenzo
- The hospitalization is in 3 days means
- An opacifying of the gastric tube remainder can be realized by oral way either with 2nd or at the 5th post-operative day (TOGD to see SCANNING TDM with oral opacifying): it makes it possible to confirm the good sealing and the absence of complications (leak-dents).
- A progressive food (mixed liquid then, pasty) is authorized starting from J1.
The dietetic follow-up is very important during the first months which follow the intervention: the weight loss is done by the reduction in the food supplies. We advise a frugivorous mode containing fresh juice of vegetables and fruits (juice extractor = centrifugal machine) during the post-operative first 15 days then a mode mixed split during 5 weeks - The patients must eat with each meal a reduced quantity being equivalent to 100-150ml (a pot of yoghurt). It is preferable to use small plates.
- The resumption of the regular physical-activity is also advised.
- The hospitalization is in 3 days means
- An opacifying of the gastric tube remainder can be realized by oral way either with 2nd or at the 5th post-operative day (TOGD to see SCANNING TDM with oral opacifying): it makes it possible to confirm the good sealing and the absence of complications (leak-dents).
- A progressive food (mixed liquid then, pasty) is authorized starting from J1.
The dietetic follow-up is very important during the first months which follow the intervention: the weight loss is done by the reduction in the food supplies. We advise a frugivorous mode containing fresh juice of vegetables and fruits (juice extractor = centrifugal machine) during the post-operative first 15 days then a mode mixed split during 5 weeks - The patients must eat with each meal a reduced quantity being equivalent to 100-150ml (a pot of yoghurt). It is preferable to use small plates.
- The resumption of the regular physical-activity is also advised. .
The follow-up of the patient is less heavy than in the other techniques. It will consist in evaluating the results in terms of weight loss in excess, reduction of the IMC (up to values of normality/ponderal overload) and of improvement even of disappearance of other serious pathologies related to obesity (standard diabetes II, arterial, turbid hypertension of the triglyceride and/or cholesterol level, syndrome of apnea of the sleep).
Your content goes here. Edit or remove this text inline or in the module Content settings. You can also style every aspect of this content in the module Design settings and even apply custom CSS to this text in the module Advanced settings.