

Definition of anal fissure
Definition
The anal fissure constitutes in frequency the second reason for proctologic consultation in the adult, after haemorrhoidal pathology.
The anal crack has the same incidence in the two sexes.
- Acute anal fissure
- often brutal d’apparition, marked by a very intense anal pain started by the saddle this pain, with type of burn/tear, can cause a constipation reflex sphinctérienne diminishes makes the examination difficult.
Symptomes
Symptoms
The symptoms of the anal crack are evocative.
The patient in general constipated.
He complains about a very sharp pain immediately after the defecation.
- This pain often lasts an hour or two and
- reappears after each saddle.
Between the saddles the patient does not suffer.
Diagnostic
The examination is difficult because of spasm sphinctérien which contracts the anal opening.
One must unpleat the anus with softness (after local anaesthesia if need be)
- one centimetre length longitudinal, more or less major ulceration, with a bottom blanchâtre (sclerous).
- generally with the lower pole of the anus (at 6 a.m.)
- examination rectal: confirm the hypertonicity of the sphincter
- Anuscopy allows to better see the crack and to specify its character.
The evolution is done by thorough with remissions.
Treatement
Surgical treatment fissures anal
The surgery of the anal crack can be proposed in the event of chronic or complicated crack, or when the pains persist in a way important or repeated in spite of a classical medicamentous treatment.
The medical care of the chronic anal crack, currently made up of nitroglycerin puts cream on topic, of botulinic injection of toxin or the blockers of the calcic channels topics nifédipine or diltiazem, in the acute and chronic crack, and fissures it in the child, can be applied with a chance of cure slightly higher than a placebo.
For the chronic crack in the adult, all the medical care is much less effective than the surgery.
Some of the studied agents most recent seem promising on the basis of single individual study (oil of clove, sildénifil and “cream of care”), but miss comparison with established drugs
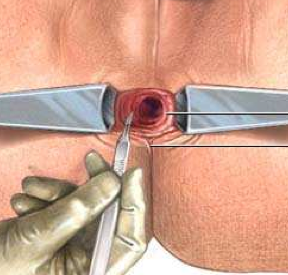
- Internal side Sphincterotomy
- It is about a partial sphinctero-leyomyo-tomy. I.e. a section partial and careful of the smooth muscle of the anus. Internal section partial sphincter anal. to release diminishes it sphinctérienne,
to decrease the pains at the time of the defecation and to secondarily allow the crack to heal.
rate of repetition < 5%
- rate incontinence with the gas (+ seepages) 8%
More than nine times out of ten, the patients operated according to this technique are satisfied
This method exposes to the risk to see appearing signs of incontinence which are usually present once on three immediately after the gesture but which they usually disappear in the weeks which follow.
The sphincterotomy proceeds, under general anaesthesia or under regional anaesthesia loco (rachis anaesthesia during which one deadens only the lower part of the body).
In the event of general anaesthesia, a Pudendal block could be associates. It be-have-to say an injection of calming directly in the sensory nerve of the anus, which will make it possible to relieve the patient the first 12 hours.
The improvement of the painful phenomena occurs rather quickly (a week).
The times of cicatrization are on the other hand longer (five weeks).
Commentaires récents