

Haemorrhoidal disease definition
Definition
Haemorrhoidal disease definition
The haemorrhoids are veins, normally located in the rectum or the anal channel.
Pathology and the symptoms are related to the dilation of these haemorrhoidal veins which increase dimension and are expressed by the anus.
The haemorrhoidal disease is source of various nuisances: red bleeding of blood accompanying or following the saddle, anal pains, dropsical pushes (swelling of the haemorrhoids), haemorrhoidal prolapse (projection of the haemorrhoids apart from the anus), haemorrhoidal thrombosis (formation of a clot in a haemorrhoidal vein).
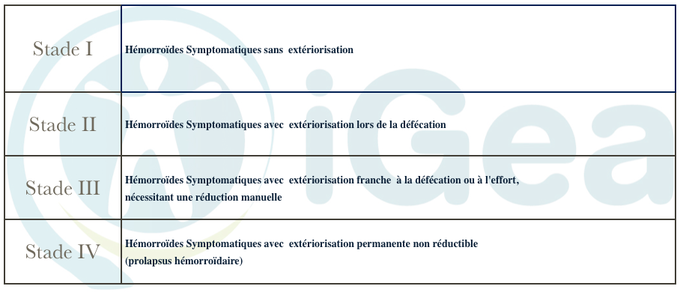
Classification haemorrhoids
Supported by the efforts of push, the haemorrhoids are classified in four stages, according to whether they remain inside the anal channel (stage 1) or that they
in leave in a permanent way (frank procidence stage 3 and prolapse stage 4).
The introduction of a treatment depends on the symptoms and the stage.
- SURGICAL INDICATION The surgery is indicated: ♦soit because of the failure of the medical care (hygiene, food mode, pomades, bindings) ♦ in urgency in the event of haemorrhoidal thrombosis ♦soit in the event of bulky haemorrhoids (stage 3 and 4)
Classification en stades de la Pathologie hémorroïdaire
Haemorrhoidal thrombosis
Approximately 15% of the patients who suffer from haemorrhoids will have pushes of thrombosis.
It is about a small generally single, bluish, hard tumefaction under the skin of the anal margin. Its spontaneous evolution is done towards one
necrose with evacuation of the thrombus or towards the slow resorption being able to lead to the formation of marisque (cutaneous after-effect).
The treatment of external, recent and painful thrombosis haemorrhoidal, is l’incision and the extraction of the clot under local anaesthesia (injection of
lidocaïne under and around the clot). An incision is carried out along the erased folds, followed by the excision of the banks to avoid their early closing. Lastly, the clot is extracted then the cavity is cleaned.
In the event of dropsical thrombosis, seen tardily, or not very painful, one resorts to the medical care associating paracetamol, AINS by oral way and
application of a pomade containing of corticoids.
| Classification pathologie hémorroïdaire dr Vincenzo Salsano Montpellier dernière mise à jours Novembre 2016 |
|---|
Causes
Surgical treatment
SOS hémorrhoïdes Montpellier : Ambulatorial surgical care
no pain method of mini invasive THD with arterial doppler ligature and mucopexy
- Method THD can be carried out within the framework from the ambulatory surgery (or 1 day surgery) with return to the residence the evening even with the monitoring of a service provider (analgesics Iv during 48 hours where necessary)
- The anaesthetist can construct a block of the pudendaux nerves with an aim of prolonging analgesia by reducing the recourse after the intervention to analgesics.
- The haemorrhoidal fabric is not removed and the anatomy of the anal channel remains unaltered. That allows the possibility of preserving the anatomical parts intended for the function of the continence.
- The intervention is almost painless because there is no ablation of fabric and the joining is made above the notched line, in a zone without sensitive nervous terminations.
- One can go back his occupation 10 days after the intervention.
- The rate of repetition is very low
- One can use it for the haemorrhoids of 2nd, 3rd and 4th stage, even bleeding
The techniques used in center IGEA of digestive surgery of Montpellier are the hemorroidectomy according to Milligan Morgan, hémorroïdopexie according to Longo and painless method mini invasive THD with arterial binding Doppler guided associated with mucopexie or face lift of the canale anal
Discuss with us in consultation to know which could be the best option for you
1) hemorroidectomy according to the technique of Milligan – Morgan modified
This classical procedure is most complete and effective technique making it possible to remove the haemorrhoids.
It is the operation most usually practised since decades.
It presents few complications and gives the best results to short and long-term.
It consists in removing the hémorroïde with the skin and the mucous membrane, until the high part of the anal channel.
Three excised are realized, corresponding to the three haemorrhoidal packages, between which “bridges” of skin and mucous membrane are spared.
That supports the cicatrization and decreases the risk of infection and stricture (contracting) anal.
2) Hémorroïdopexie according to Longo
This procedure, called hemorroidectomy with fastening, blocks blood circulation with haemorrhoidal fabric.
Fastening implies generally less pain than classical hemorroidectomy and allows a faster return to work.
However, in comparison with hemorroidectomy Milligan Morgan, fastening according to Longo was associated with an increasing risk of repetition and rectal prolapse
3) Surgical cure of the haemorrhoids into ambulatory according to painless Method mini invasive THD with arterial binding Doppler guided associated with mucopexie
| traitement chirurgical des hémorroïdes dr Vincenzo Salsano Montpellier dernière mise à jours septembre 2016 |
|---|
Methode THD
SOS Hémorroïdes
THD méthode indolore pour la cure des hémorroïdes
This innovating and painless method allows a fast return to normal activities for a pathology attends whose treatment was always regarded as handicapping and painful.
It is about a surgical device of sterile single use which understands a anuscope with sliding operational window (passage of the door switches), a sensor Doppler of single use, a lighting system with optical fiber.
The intervention of THD is based on 2 concepts: 1) the desarterialisation and 2) the mucopexie or face lift
- Désarterérialisation
- ♦DIMINUTION OF THE BLOOD-PRESSURE ON THE LEVEL OF THE ANAL CHANNEL
- ♦Identification and selective binding of the 6 terminal sections of the higher rectal artery. The 6 branches are located by Doppler echography and then bound by joining résorbable ♦ desarterialisation relieves congestion the haemorrhoidal cushions and corrects the bleeding
- Mucopexie or face lift of the anal channel
- ♦REDUCTION OF THE PROLAPSE BY FACE LIFT OF THE ANAL CHANNEL The points of desarterialisation are used as fixing for a plicature of the prolapse in overcasting. That makes it possible to position back the haemorrhoidal cushions in their anatomical seat
Benefit THD
1) Minis invasive and nontraumatic
2) Feasible in ambulatory surgery
3) Marginal post-operative pain
4) Very fast re-establishment
5) Wide indications
6) No serious complication
BIBLIOGRAPHIE THD 1
Operated patient testimonies of cure of the haemorrhoids
with method THD
| THD méthode indolore pour la cure des hémorroïdes dr Vincenzo Salsano Montpellier dernière mise à jours Février 2013 |
|---|
Postoperative follow-up
Postoperative follow-up
One supervises the postoperative Pain, the resumption of Minction, the postoperative Bleeding, the resumption of the Transit
Pain after hemorroidectomy or hémorroïdopexy
- To reduce the operational pain post after hemorroidectomy in our technique we use scissors either ultrasonic or bipolar
- The antalgic treatment/anti-inflammatory drug is systematically managed during the first postoperative days
- The pain is revived at the time of the first saddles after hemorroidectomy.
- This treatment is supplemented by tramadol or derivatives of morphine per os or by way under cutaneous
Normal micturition after hemorroidectomy or hémorroïdopexie Us you demandon to urinate before the intervention. - It is important to prevent this risk of vesical sphere by privileging the general anaesthesia with the rachianesthesy.
- A retention of urine is source of pains sometimes difficult to specify.
- At the man, the administration of antispasmodic and agents blocking alpha 1 must be under consideration before the vesical survey.
- A simple evacuation survey is enough at the woman.
Bleeding after hémorroïdectomieou hémorroïdopexie
- A bleeding of low abundance, at the time of the first saddle is frequent and nonworrying.
- A haemorrhage with emission of clots can occur in the first hours or days, some is the procedure, mainly during the first two weeks.
- In the event of haemorrhage, a local plugging can be enough.
- In less than 3% of the cases it will be necessary D to operate in urgency to carry out a gesture of hémostase to the surgical unit under general anaesthesia.
First Saddles after hemorroidectomy or hémorroïdopexie
- The laxatives are systematically continued into postoperative in order to obtaining a first saddles soft in the 48 to 72 hours.
- In the event of hemorroidectomy, it is advised to take analgesics before the first defecation and not to be locked up in the toilets (risk demalaise vagal). The following saddles are less and less painful on condition that drinking much water and continuing the catch of laxative in order to obtain soft saddles.
- The pains generally disappear after the course from the 10th day.
| Suivi Postopératoire après cure d’hémorroïdes dr Vincenzo Salsano Montpellier dernière mise à jours Novembre 2016 |
|---|
Complications after cure haemorrhoids
Complications
Postoperative complications after cure haemorrhoids
Complications after hemorroidectomy according to Milligan Morgan or hémorrhoïdopexie according to Longo
are not very frequent
They consist of 4 possible but rare events: hémorrhagie postoperative, abscess, anal stricture, haemorrhoidal repetition.
Postoperative Hémorrhagie after cure haemorrhoids
A bleeding can occur in the first hours following the intervention and requires a surgical gesture of hémostase (2% of the cases).
The bleeding can also make following the fall of a scab of cicatrization (around the 10th post-operative day), and must encourage to consult in urgency to judge need or not for a surgical hémostase.
To prevent this risk we use ultrasonic scissors (at the cost of an increase in the costs direct of the operation) or bipolar scissors
Postoperative abscess after cure haemorrhoids
The infection of the operated area is very rare.
A systematic antibiotic treatment during and after the operation, and this during 48 hours.
Postoperative anal stricture after cure haemorrhoids
The stricture (contracting) of the anus occurs in literature in 4% of the cases.
It is exceptional if the postoperative care is well followed.
This stricture, awkward and difficult to treat, must be prevented by the daily practice of a rectal examination by your care, using a fingerstall petroleum jelly, as soon as possible and until the post-operative consultation (at the end of one month).
If the realization of this touch is impossible because of too intense pains, you must renew contact with us to carry out a dilation under a short general anaesthesia.
Haemorrhoidal repetition
The repetitions concern less than 1% of the patients.
At the time of one only operation one cannot remove, entirely, haemorrhoids circumferential and very bulky.
For these reasons, only the haemorrhoids bulkiest are réséquées.
The final result will be judged after 3-4 month as well as the indication of a complement of exérèse.
Commentaires récents