

– – Cancer of the right colon : Définition
Definition
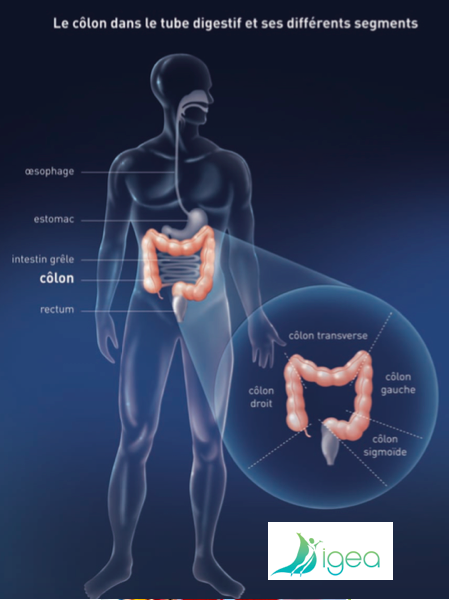
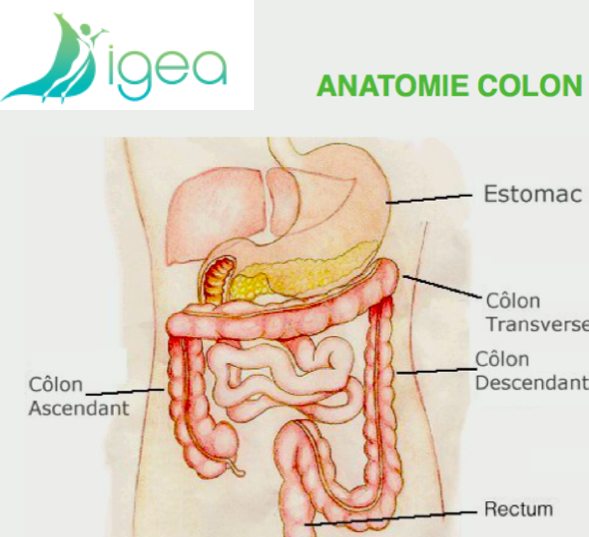
The cancer of the right colon is localised in the right part of the colon who goes from the caecum to the angle right colic.
This surgical pathology is treated with a right hemicolectomy.
It is about a resection of the right colonist, with re-establishment of digestive continuity.
It is carried out thanks to a joining (= anastomosis iléo transversee) between the distal small intestine and the transverse colonist
– – Risk factors
Risk factors cancer right colon
- Polyps
- Between 60 and 80% of cancers of the colon develop on précancéreuses benign tumours: polyps or adenomata. The frequency of these lesions increases regularly with the years. According to the observations collected at the time of autopsies, 12 % of the people of less than 55 years are reached by it.
- age
- Rare before 40 years, cancers of the colon
- heredity
- All in all, the existence of a cancer in a relative of the first degree would multiply by two the risk of cancer.
- family forms
- Certain family diseases involve a main risk of cancer of the colon. It is in particular the family adénomateuse polypose, which are characterized by the early appearance of multiple polyps on all the colon, and the syndrome of Lynch. The early development of a cancer is inescapable in the event of polypose family In the syndrome of Lynch, the risk is extremely high, but a little later. It is associated an increase with the frequency of cancers of the endometer like, to a lesser extent, other cancers (stomach, ovary, urinary tracts…).
- inflammatory diseases of the intestine
- The influence of the disease of Crohn on the cancer of colon remained discussed a long time. The ulcéro-hemorrhagic rectocolite is a classical risk factor of cancer colorectal. However, the risk is function of the extent of the attack colic and its seniority Today, it seems clear that this disease is also an important risk factor when it reaches all the colon and that it began in young age.
- Supplies
- Other risk factors of cancer of the colon were evoked, such as a food low in fibres and rich in grease.
In addition certain data suggest that the chronic anti-inflammatory drug catch not stéroïdiens could play a protective role. But these factors remain very discussed
– – Surgical treatment of Right Hemicolectomy
Right Hemicolectomy
- Operational indications
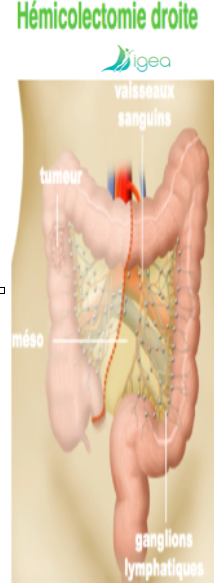
- ◊ Cancer of the right colon: caecum, ascending colon, angle right colic ◊ Polyp colic not résécable by endoscopy ◊ Disease of Crohn reaching the iléon (small intestine terminal)
- The carcinological intervention comprises a exérèse carrying the end of the last handle iléale and the colonist until one the right third of the transverse. It is necessary to carry out a binding first of the right vessels colics higher, colics means, and ileo-caeco-colo-Appendicularia in contact with the higher axis mesenteric. The re-establishment of continuity is carried out in same time with anastomosis iléo-transverse termino-final or termino-side
The intervention can be realized
- by a traditional technique
- maybe by laparoscopy (mini invasive, closed belly)
The operational act is longer in coelioscopy than in open surgery.
The resumption of the transit and the food is probably faster after right colectomy by laparoscopy (coelioscopy).
The duration of hospitalization is probably not very different according to the technique used.
The carcinological quality of the resection and postoperative quality of life are not different for the laparoscopy (coelioscopy) and the open surgery.
For the disease of Crohn, there exists an important benefit parietal and aesthetic related to the use of the long-term coelioscopy (young patients and iterative interventions).
– – Complications after Hémicolectomie right-hand side
Complications after Hémicolectomie right-hand side
COMPLICATIONS
- They are rare.
- It is about a surgery frequently carried out.
- The technique, either by laparoscopy, or by opened way, is standardized, sour and reliable.
The anastomotic leak is major complication after resection colic
The risk of dent is estimated between 1% and 3%. It is about a matter escape through the joining colic because the joining is not tight.
This dent can involve a post-operative peritonitis, which imposes a reintervention in urgency and sometimes the clothes industry of a double stomy on gun of rifle (artificial anus) with disassembling of anastomosis
Obstruction of the bowels
A difficult resumption of the transit can make necessary the realization a scanner to eliminate diagnoses it postoperative obstruction of the bowels on support or internal hernia (imprisonment of a handle of hail in a breach created by the intervention).
L’abcès of walls is rare after laparoscopic surgery
Other risks are inherent in any act of abdominal surgery: 1) iatrogenic attack/wound of another abdominal body 2) haemorrhage…
Anticoagulants are prescribed to reduce the risk of phlebitis and/or pulmonary embolism.
– – Symptoms
Symptoms of the right colon cancer
The cancer of the right colonist can develop for one long period of time without no sign/symptom appearing. When the symptoms appear, they are often vague and can be confused with those of more current disorders. It is important to consult a doctor.
- Symptoms cancer right colonist
- méléna or of the rectorragies? presence of blood on or in the saddles (of very dark color or bright red) tiredness related to anaemia – usually following the bleedings on the level of the intestine weight loss or general state deterioration diarrhoea, constipation or both, in alternation: saddle unusual (during one prolonged period) revealing complication of the tumour of the right colonist: 1) obstruction of the bowels or perforation (infectious complication with type of abscess perineoplasic) 2) metastatic liver
Diagnostic and Therapeutic Pre Assessment
The diagnosis of the cancer of the colon rests on the coloscopy which makes it possible to visualize the tumour, to carry out biopsies and to search
synchronous lesions (of the rectum and left colon)
The therapeutic pre assessment of a cancer of the right colon must comprise research
visceral metastases by a hepatic echography and possibly an abdominal examination scanographic thoraco.
The proportioning of ACE is useful to supervise the evolution after treatment.
– – Useful info
Right Colectomy
Surgical consultation Colectomie Right
The surgeon digestive explained you holding them and the outcomes of the right colectomy which is necessary in your case
The operational date was scheduled.
right colostomy = information useful to know
An appointment near the anaesthetists was agreed (think of filling out the medical questionnaire for our fellow-members)
A regulation d’ORAL IMPACT will be delivered to you: to begin 7 days before the intervention. This oral supplementation is a drug the purpose of which is to decrease the operational complications post, by increasing your immunizing defenses. • In the event of laparotomy, a belt of abdominal application will be prescribed to you (think of bringing it the day of the intervention)
An enlightened assent: to supplement, sign and give before the hospitalization.
An estimate if going beyond fees: To send to your mutual insurance company (preliminary agreement for refunding). ◦
An invoice will be given to you to your exit, allowing you refunding by your mutual insurance company.
A form to book a particular room or a single room. The particular room can be proposed only according to the places available.
Right intervention day before of Colectomie
You will be hospitalized (E) the day before intervention around 4 p.m. with the private clinic and will be accommodated (E) by ancillary medical staff
YOUR TITLE
Need for making the administrative entrance with the service ADMISSION and after you Go up in the service where you will be accommodated (E) by the nurse.
To specify with L ` nurse your wish to be transferred (E) secondarily in Convalescent home, following your hospitalization, before turning over definitively to your residence.
Not to forget to check with it the phone number of the trustworthy person, with whom the surgeons will be able to discuss.
To give to the nurse your file of entry, the lit assent, results of blood and morphological examinations, the belt of application in the event of laparotomy
Visit of the anaesthetists and the surgeons
Shower disinfectant (discussion with auxiliary nurse).
Meal the evening, then with jeun as from midnight.
In the absence of operational pre coloscopy, no purging, nor rectal injection will be proposed to you
Surgical unit the following day in the course of the day.
The intervention of colectomy and your hospitalization with the private clinic
The intervention of the colectomy hard Right approximately of 1 a.m. 1? 2 to 3 a.m. This intervention is carried out under general anaesthesia.
Rachis anaesthesia will be proposed to you: they are anaesthetic injections, directly on the level of the spinal column. The rachis anaesthesia make it possible to decrease any operational pain post.
This one is often proposed, in the case of right colectomy by laparotomy.
During the intervention, he will be set up a perfusion, that is to say by peripheral way or center lane, as well as a urinary probe by way naturale or known pubic (= we prefer the cystocath at the men)
Colostomy droitePostopératoire
In post operational, you will be awaked (E) in recovery room, then secondarily transferred (E): in the surgery department or the service of intensive care surgical.
Your intensive passage in care will be determined by the surgeon and the anaesthetist: this stay makes it possible to carry out a better monitoring, and thus to regulate, as soon as possible, a possible complication. You will be thus under monitoring monitoring (pulse, tension, heart rate, temperature, diuresis and assessment).
Concerning the information of the families, will know that the surgeon is at your disposal the evening after the consultation every afternoon.
The evening of your intervention, you will remain with jeun, with drugs, against the pain, managed by venous way and/or rachis anaesthesia
The following days, after agreement of the surgeon, you will be, transferred (E) that is to say in your room alone (or double).
The food will be carried out gradually and the treatments will be managed by the mouth.
A prevention of the phlebites and gastric protection will be systematic.
Exit of the Private clinic after Colectomie right
In the event of return to residence, you will leave the private clinic, at the end of the morning
A report of hospitalization (+ operational report) will be systematically addressed to your attending physician and all to the correspondents (gastro-enterologist, cancer specialist…).
Exit of the Private clinic
Ordinances of analgesics and Heparin with low molecular weight (HBPM) in order to avoid any secondary phlebitis and pulmonary embolism
An ordinance of nurse in residence, for the injections of Heparin and possible local care.
A sick leave will be given to you if necessary. You will thus have at disposal
A belt of application, in the event of surgery by laparotomy.
An appointment with the surgeon
It is recommended to you to go, to avoid the wearing of heavy load.
The showers are authorized as of the return to residence, in the absence of local care, on the level of the wall.
It will be necessary to wait about fifteen days for the catch of baths out of fresh water or swimming pool.
With regard to the food, it no specific scheme to be envisaged there, but it is necessary to adapt the food according to the transit namely: good hydration, fruit and vegetables if constipation; pastes and rice if diarrhoea.
Indeed, you will have the transit disturbed during 3 to 4 months.
In the event of transfer in convalescent home, all the medical documents will be directly transmitted to the structure concerned.
In any event, will know that in the event of carcinological surgery, your dossier will be presented and discussed in multidisciplinary meeting with surgeons, radiologists, gastroenterologists and cancer specialists
According to the histological result of the operational part, a possible chemotherapy will be proposed to you.
Commentaires récents