

Treatment of an eventration

Definition
Hernia along an old scar or post-operative eventration.
An eventration is a hernia which develops along a scar of a laparotomy (incisional hernia).
It is a parietal defect (aponeurotic dehiscence with peritoneal sac/pouch) in 95% of cases, as a consequence of surgery, and for the remaining 5%, following a trauma.
The large majority form and become apparent during the year following the initial surgery.
Eventrations are frequent, affecting 5 – 20% of operations with classic incisions of the abdomen (laparotomy)
Symptoms
The most frequent eventrations are painless and capable of being reduced.
An eventration looks like an arched bulge or localised mass on an old abdominal scar.
It can contain part of the small intestine or the large intestine, and sometimes both at the same time.
The progressive development of the sac/pouch, and the increased heaviness of its contents, are a source of discomfort which could become debilitating.
An eventration which becomes painful may turn into something more complicated, such as an intestinal occlusion (the intestine is blocked in the hernia) with the risk of intestinal perforation.
The signs of an occlusion are the absence of gas and matter, and are sometimes associated with vomiting.
Surgery is necessary and urgent.
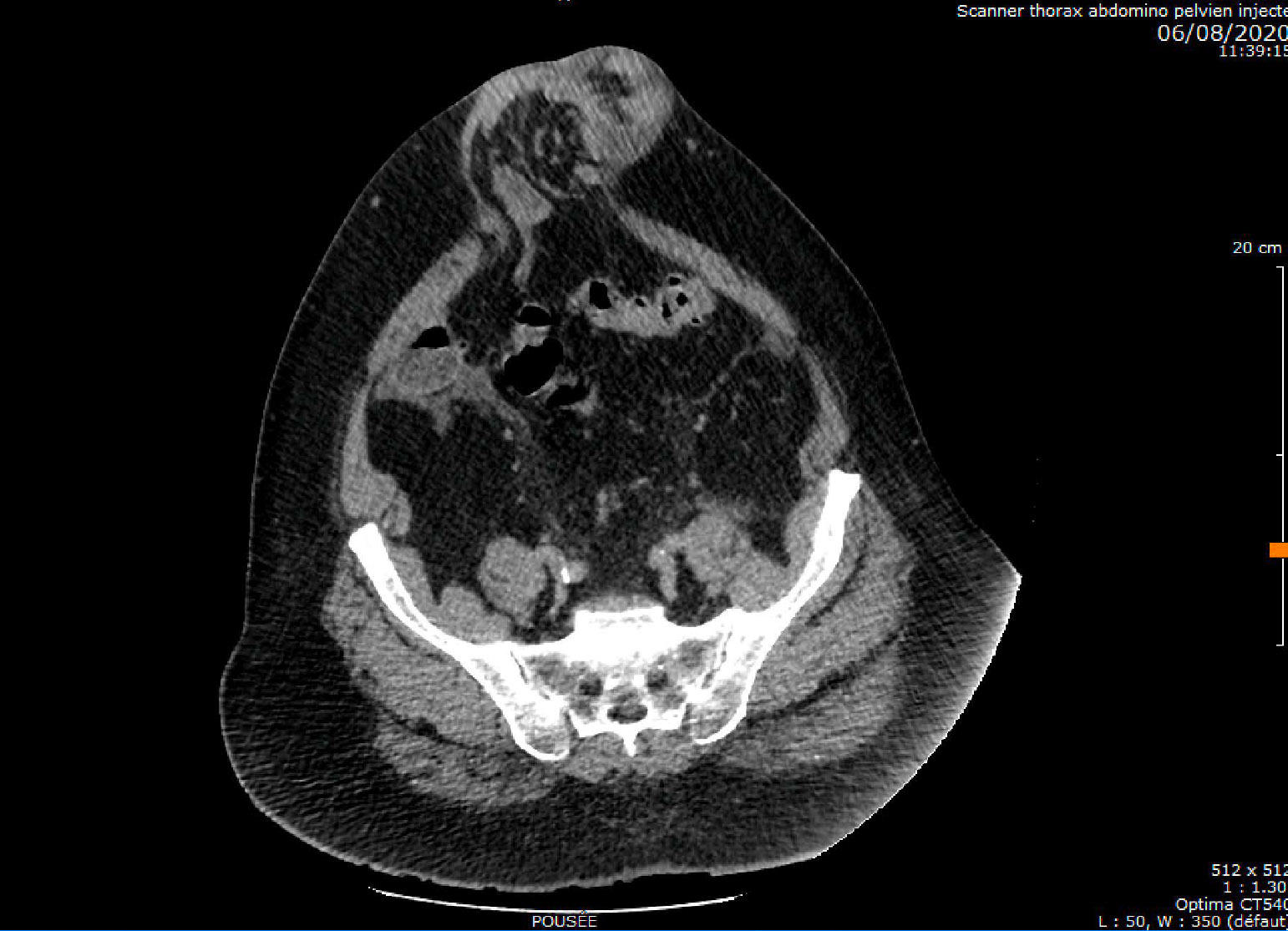
scannography of an eventration
Symptoms:
- Pain.
- Intestinal occlusion (strangulated eventration).
- Intestinal perforation (gangrene).
- Breathing problems if the person has a large eventration.
Two examples:
- Large eventration with moveable contents: It causes paradoxical abdominal breathing, which in turn creates respiratory insufficiency.
The diaphragm is permanently relaxed and the intra-abdominal pressure is low.
- Large eventration with a fixed content: The intestines are contained in a peritoneal sac/pouch outside the abdomen (the second abdomen of Goni Moreno). Surgical treatment is delicate as reintegrating the intestines provokes respiratory imbalance.
Causes and Risk Factors for eventration
Type of incision (> risk) :
- Midline laparotomy: midline incisions are more likely to make complications for the eventration, compared with transverse or oblique incisions.
- Iterative laparotomy.
- Site of a colostomy.
- Multiple drainage orifices.
- Bullet or knife wounds: muscle damage and infection
Risk factors:
- Obesity.
- Post-operative infection: abscess or abdominal wall haematoma.
- Pulmonary complications, with congestion and difficulty coughing.
- Post-operative abdominal hypertension factors.
- Spreading.
- Immunodepression treatment (corticosteroid therapy and chemotherapy)
- Malnutrition
The best way to avoid eventration is the development of keyhole surgery and thereby avoiding large, classic incisions.
Surgical treatment
Surgical treatment for an eventration with a mesh prosthesis implant:
Indications :
Eventrations whose volume is increasing must have surgical treatment as they are very uncomfortable and moreover very painful. Very often they are the precursor of a strangulated eventration.
The post-operative treatment of eventrations of the anterior abdominal wall consists of dissecting the hernia sac/pouch, and reintegrating the intestine into the abdominal cavity then repairing the abdominal wall with, or without the implant of a mesh prosthesis.
The treatment can be either anterior (laparotomy) or intraperitoneal (keyhole surgery).
Surgery treatment for an eventration with the fixation of a mesh prosthesis (anterior):
- The old scar is resected.
- This surgical operation requires a vast detachment and extended dissections. It can last between 1 and 3 hours, depending on the case.
- The musculo-aponeurotic edges are perfectly dissected in order to present on each side tissue which is healthy and solid (surgical trimming of wound edges).
- Haemostasis is meticulous in avoiding post-operative haematomas.
- Parietal repair is possible due to a mesh prosthesis.
- The prosthesis is placed behind the pre-facial muscles, between the peritoneal plane and the fascia plane using the tension free technique.
- In certain rare cases, the space between the peritoneum and the muscles is inaccessible or unusable. A double phase mesh prosthesis must be placed in the peritoneal cavity. The mesh must not adhere to the intestine.
- The surgery often ends with aspirative drainage in the subcutaneous space (Redon drain).
- These prostheses are perfectly tolerated by the organism, and no allergic phenomena exist.
Complications with eventration treatment:
- Haematoma.
- Recurrent.
- Infection of the mesh (0.5-1% ): however, once an infection is present, the whole of the mesh must be removed. This is necessary to allow recovery.
Keyhole surgery
Eventration treatment by keyhole surgery with the intraperitoneal installation of a prosthesis mesh.
The surgeons of the iGEA team are specialised in eventration treatment by keyhole surgery.
Advantages :
- Only slightly aggressive.
- Less post-operative pain.
- Early return to physical activity.
Contraindications for keyhole surgery:
- Strangulated eventration
- Size of the neck of the eventration greater than 6cm in diameter.
Useful information
Complications with eventration treatment with implant of mesh prosthesis by the classic method.
A precise evaluation of the risks is essential before the surgery takes place.
A consultation with a Pulmonologist for a pulmonary function evaluation is obligatory for large eventrations (post-operative respiratory physiotherapy).
If the patient has excess weight, a weight-loss programme is always recommended.
Please Note:
- You will check in to the clinic either the night before, or the morning of the operation.
- Do not forget the anti-thrombosis stockings (prescription supplied during the consultation).
- Do not forget the compression belt adapted to your waist size (prescription supplied during the consultation).
- You must indicate any known skin allergies (especially to iodine).
- You will be given antibiotics during and after the surgery.
- Blood loss is usually very small, and no transfusion is necessary.
- The mesh prosthesis is placed deeply under the skin tissue, is not perceptible and will cause no discomfort.
- The removal of the aspirative drainage system (Redon) takes place between 2 and 4 days after the operation. They are placed in the detachment area between the mesh prosthesis and muscles, and under the skin.
- Food and drink are allowed the evening of the operation or the following day.
- Normally, pain is not very intense, nevertheless, painkillers are always provided.
- The stitches will be removed between 8 and 15 days after surgery.
- You can take a shower as soon as the drainage system is removed.
- Depending on the gravity of the surgery, you will leave the clinic between 2 and 6 days after the operation.
Important :
- During one month it is not recommended that you undertake any strenuous physical efforts.
- Wait for 3 months before doing intense, physical effort, with sudden violent bursts, and to return to normal physical and sports activities.
- The period you will be unable for work, depends on the size of the eventration, and your type of work: it could be from 7 to 49 days.
Riferimenti bibliografici
- Reference 1 : Test1
- Reference 2 : Test
- Reference 3 : Test
- Reference 4 : Test
- Reference 5 : Test
- Reference 6 : Test
- Reference 7 : Test
- Reference 8 : Test
- Reference 9 : Test